When Medicine Has No Roadmap: A Documented Case of Rapid Recovery From Ciguatera Poisoning
Jose returned from a fishing trip in Cancun expecting nothing more than vacation photos and fond memories. Instead, within hours of one celebratory meal, he found himself battling severe nausea, debilitating confusion, and intense itching that left local doctors baffled.
When he contacted Direct Med Clinic, something unusual happened: his symptoms improved dramatically within 24 hours of targeted supportive care. This is his documented case story.
Quick Facts: What You Need to Know About Ciguatera
What it is: Foodborne illness caused by ciguatoxin, a heat-stable marine toxin found in certain reef fish
Common fish carriers:
- Barracuda (highest risk)
- Mahi-mahi
- Red snapper
- Grouper
- Amberjack
Key symptoms:
- Gastrointestinal: Nausea, vomiting, diarrhea, abdominal pain
- Neurological: Tingling, severe itching, cold-hot reversal, brain fog
- Cardiovascular: Slow heart rate, low blood pressure
Timeline: Symptoms appear within 6 hours, can last days to months
The medical challenge:
- No FDA-approved cure
- No standardized diagnostic test
- Most U.S. mainland clinicians have never treated a case
What Jose Experienced: A Classic Presentation
Jose’s symptoms began suddenly after eating barracuda during his trip. Within hours, he developed:
- Severe gastrointestinal distress that wouldn’t subside
- Significant itching and unusual sensory disturbances
- Cognitive difficulties including brain fog and confusion
- Fluctuating neurological symptoms that changed hour by hour
When he sought care locally, providers ran standard tests but couldn’t connect his symptoms to a clear diagnosis. The toxin doesn’t show up on routine bloodwork. His presentation didn’t fit common food poisoning patterns. And because ciguatera is rare in the continental U.S., it wasn’t on most clinicians’ radar.
Tests came back normal. He was discharged without answers. But the symptoms persisted — and in some ways, worsened.

Why Ciguatera Is So Difficult to Diagnose
Ciguatoxin is a naturally occurring marine toxin produced by microscopic algae in coral reef ecosystems. Small reef fish eat the algae, larger predatory fish eat those fish, and the toxin accumulates up the food chain through a process called bioaccumulation.
What makes it particularly challenging:
- The toxin is invisible: Odorless, tasteless, and not destroyed by cooking, freezing, or any food preparation method
- Symptoms vary widely: Some patients experience primarily GI symptoms, others mainly neurological, and many have both
- No standard test exists: Diagnosis relies entirely on clinical presentation and patient history
- Most U.S. providers lack experience: While common in Hawaii, the Caribbean, and Pacific islands, mainland physicians rarely encounter it
The biological mechanism: Ciguatoxin binds to voltage-gated sodium channels in nerve and muscle cells, causing prolonged channel opening. This leads to neurological hyperexcitability, disrupts normal cellular signaling, and generates significant oxidative stress in affected tissues.
For patients like Jose, this means navigating a healthcare system that isn’t equipped to recognize what they’re experiencing — much less treat it.
The Direct Primary Care Difference: Time to Think and Research
When Jose contacted Direct Med Clinic, the response looked fundamentally different from his previous care experiences.
What the DPC model enabled:
- Immediate access: He reached his clinician directly, after hours, when symptoms were most severe
- Time to research: Instead of a 15-minute appointment, the care team had freedom to dive deep into medical literature on ciguatoxin mechanisms and published case reports
- Protocol development: Based on the toxin’s known biological effects, the team designed a targeted supportive care approach
- Daily monitoring: Through direct communication channels, providers tracked his symptoms in real-time
- Responsive adjustments: As symptoms evolved, the care plan adapted immediately
This is what makes Direct Primary Care different: when standard protocols don’t exist, clinicians have the time and freedom to think critically, research thoroughly, and respond immediately.
The Clinical Approach: Research-Based Supportive Care
Because of the DPC model’s flexibility, Jose’s clinician had time to:
- Review published case reports on ciguatera treatment approaches
- Study the toxin’s mechanism of action at the cellular level
- Research supportive therapies that address oxidative stress
- Design a monitoring protocol to track response
The clinical rationale for IV glutathione:
Given that ciguatoxin generates significant oxidative stress in affected tissues, the team considered high-dose antioxidant therapy as a supportive intervention.
Glutathione is:
- The body’s primary intracellular antioxidant
- Commonly used in clinical settings for toxin-related oxidative stress
- Well-documented for supporting cellular redox pathways
- Available for IV administration at therapeutic doses
This was an off-label, research-informed clinical decision made with full patient consent and supported by real-time monitoring.
The Documented Outcome: Rapid and Significant Improvement
The supportive care plan included:
- High-dose IV glutathione infusion
- Symptomatic medication for itching
- Structured daily symptom tracking
- Close communication throughout recovery
What happened after the first IV glutathione treatment:
Jose reported approximately 50% reduction in overall symptoms within 24 hours, including:
- Noticeable cognitive improvement and clearing of brain fog
- Significant reduction in itching intensity
- Ability to function normally and return to work the following day
- Meaningful restoration of daily work capacity
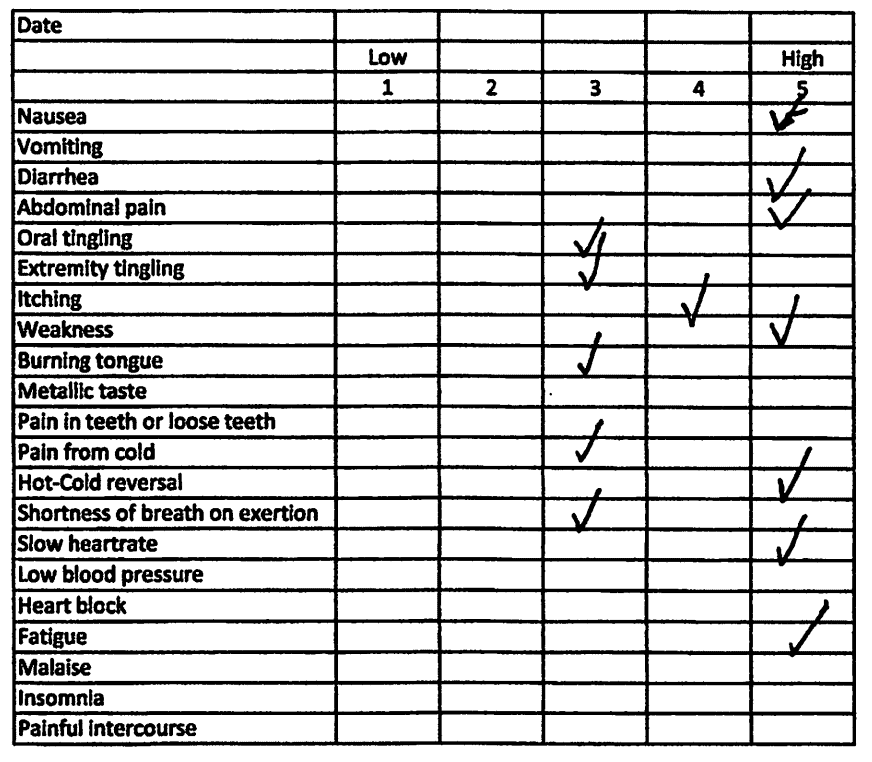
These changes were documented using a structured symptom-tracking sheet that measured:
- Neurological symptom severity
- Gastrointestinal symptom progression
- Cognitive function markers
- Overall functional capacity
Important context: This documents one patient’s experience with a specific supportive care protocol. This does not establish glutathione as a cure for ciguatera poisoning, nor does it guarantee similar outcomes in other cases. However, the rapid and measurable improvement in this documented case suggests that targeted antioxidant therapy may warrant further investigation for ciguatoxin-related oxidative stress.
Why Documentation Matters for Rare Conditions
The detailed symptom tracking in Jose’s case showed:
- Clear temporal relationship between intervention and improvement
- Stabilization across multiple symptom categories
- Progressive improvement over subsequent days
- Quantifiable changes in functional capacity
When conditions fall outside conventional medical experience, rigorous documentation transforms a patient story into case report-level data. This kind of systematic tracking:
- Provides objective measures of symptom changes
- Reduces uncertainty for patients navigating recovery
- Supports clinical decision-making with real data
- Builds institutional knowledge for future similar presentations
- Creates educational content for other clinicians
In rare toxin cases, every documented outcome contributes to the broader medical understanding of what interventions may help when standard treatments don’t exist.
The Science Behind the Approach
Understanding ciguatoxin’s mechanism helped guide treatment decisions:
Ciguatoxin causes:
- Prolonged opening of voltage-gated sodium channels
- Neurological hyperexcitability throughout the nervous system
- Disrupted cellular signaling
- Significant oxidative stress in affected tissues
Glutathione’s potential role (case-specific rationale):
- Acts as a high-dose antioxidant at the cellular level
- Supports the body’s natural redox pathways
- May help address toxin-related oxidative damage
- Has established safety profile in clinical use
This biological framework provided a rational basis for the supportive care approach, even in the absence of FDA-approved protocols.
What Standard Healthcare Couldn’t Provide
In a conventional medical setting, Jose’s case would likely have followed this path:
- Emergency department visit with standard workup
- Normal test results leading to discharge with “suspected food poisoning”
- Multiple follow-up appointments as symptoms persisted
- Possible referrals to specialists (GI, neurology)
- Weeks of fragmented care with no coordinated treatment plan
What was missing: Time for research, ability to implement novel supportive protocols, daily monitoring capacity, and direct communication channels.
Standard clinics cannot offer:
- After-hours direct access to clinicians
- In-depth research time on rare conditions
- Rapid protocol development and adjustment
- Daily symptom monitoring
- Continuous communication throughout recovery
The DPC model makes all of these standard practice rather than exceptional circumstances.
Travel Medicine Lessons: What You Should Know
If you’re traveling to tropical regions:
- Avoid barracuda and large predatory reef fish
- Ask locals which fish are considered safe in that specific area
- Remember that ciguatoxin can’t be detected by appearance, smell, or taste
- Even fish from the same catch may have varying toxin levels
If you develop symptoms after eating reef fish:
- Document exactly what fish you ate and when
- Track the timing and type of symptoms carefully
- Seek medical attention and specifically mention “ciguatera poisoning” as a possibility
- Be prepared that initial tests may come back normal
- Keep detailed symptom logs to help clinicians track patterns
During recovery:
- Avoid alcohol, nuts, fish, and caffeine (may worsen neurological symptoms)
- Stay well-hydrated
- Expect neurological fluctuations — recovery is rarely linear
- Be patient — some symptoms can persist for weeks or months
The Documentary: Bringing the Science to Light
A short documentary currently in production will feature:
- Direct footage and interviews with Jose
- The actual symptom-tracking sheet used during treatment
- Dr. Moczygemba’s clinical reasoning and research process
- The biology of ciguatoxin and its effects on human physiology
- The supportive care protocol and treatment timeline
- The documented response to IV glutathione therapy
The focus is educational: How can clinicians approach rare toxin exposures when no approved treatment protocol exists? What role can systematic documentation play in advancing medical knowledge? How does the Direct Primary Care model enable this kind of personalized, research-driven care?
This isn’t promotional content. It’s an honest examination of what becomes possible when clinicians have time to think, research, and respond to medical complexity.
What This Case Means for Modern Primary Care
Jose’s documented improvement highlights a fundamental challenge in modern healthcare: the system works well for common, straightforward conditions but struggles with anything that falls outside standard protocols.
Rare toxin exposures, unusual presentations of common diseases, complex chronic conditions, and diagnostic mysteries all require the same things:
- Uninterrupted time to research and think
- Freedom to investigate beyond the obvious
- Continuity of care across the illness trajectory
- Direct communication without administrative barriers
- Clinicians empowered to practice real medicine
The Direct Primary Care model doesn’t just make these things possible — it makes them the default.
In Jose’s case, this translated to:
- Same-day protocol development based on toxin biology
- Real-time symptom tracking and response monitoring
- Rapid clinical decision-making when he experienced improvement
- Continuous availability throughout the recovery process
These capabilities aren’t luxuries. For rare conditions, they’re essential.
Implications for Ciguatera Treatment
While one documented case doesn’t establish a treatment standard, Jose’s rapid response to IV glutathione therapy raises important questions:
- Could targeted antioxidant therapy help other ciguatera patients?
- What role does oxidative stress play in symptom severity and duration?
- How can we better document and share outcomes in rare toxin cases?
- What other supportive approaches warrant investigation?
The medical community needs more data, more documented cases, and more clinicians willing to carefully track outcomes when they encounter these rare presentations.
That’s exactly what Direct Med Clinic is building: a systematic approach to documenting and sharing knowledge about conditions that fall outside conventional treatment pathways.
Why We’re Sharing This Story
At Direct Med Clinic, we believe medical knowledge grows when clinicians openly share what they learn — including successful outcomes and the clinical reasoning behind them.
Jose’s case taught us:
- How ciguatera presents in returning travelers
- The value of detailed, systematic symptom tracking
- That targeted supportive care based on toxin biology may offer benefit
- What’s possible when providers have time to truly engage with medical complexity
We’re not claiming to have discovered a cure for ciguatera. We’re sharing a documented case of significant improvement after research-based supportive care, in the hope that it contributes to the broader medical understanding of how to help patients when standard protocols don’t exist.
If you’ve exhausted your options elsewhere, if your symptoms don’t fit standard patterns, or if you simply want a provider who has time to research, monitor, and respond — that’s exactly what Direct Primary Care was designed for.
Recent Comments